
Introduction
Machines offering ultraviolet-C (UV-C) light for the high-level disinfection of medical devices are rapidly emerging worldwide. This surge in the use of UV-C requires healthcare practitioners to take extra precautions before embedding unconventional technology into standard procedures.

What is UV-C?
Ultraviolet-C radiation is a wavelength of light that falls between the spectrum of X-rays and visible light. Light within this range has been shown to inactivate certain microorganisms through a specific reaction pathway. This is typically achieved using low-pressure mercury lamps. However, recently, LED lamps have been utilised as an alternative.
Ultraviolet (UV) light destroys microorganisms by targeting the DNA or RNA within microorganisms. This causes a photochemical reaction, creating abnormal links within the DNA or RNA. The chemical structure is distorted which interferes with the normal function of the microorganism, leading to mutations or inactivation.
How is it used?
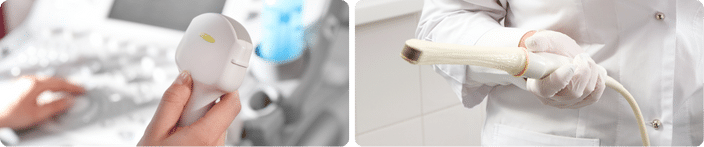
UV light is used in various settings, including water treatment systems and piping networks, as well as healthcare and food industry settings, including the disinfection of ventilation systems, surfaces, and devices. Its use in healthcare is becoming increasingly common, particularly for the disinfection of non-lumened, semi-critical medical devices.
A typical UV-C machine comprises a hard plastic cabinet housing multiple UV lamps within a mirrored glass chamber. A portion of the medical device is hung inside the chamber, with the door closed to protect the end user, and UV-C light is emitted onto the device.
The Spectrum of Light

This article outlines six critical considerations before adopting UV-C technology for your hospital medical device decontamination procedure.
1. Lack of Standardisation and Data

EN 14885 Chemical disinfectants and antiseptics - Application of European Standards for chemical disinfectants and antiseptics plays a crucial role in ensuring the efficacy, safety, and quality of chemical disinfectants and antiseptics used in various settings, including healthcare. Chemical disinfectants in Europe and the UK follow this guidance as it specifies the requirements for the testing of chemical disinfectants and antiseptics to support the antimicrobial claims they make. (Bolten, Schmidt and Steinhauer, 2022)1
The standardisation of disinfectant test methods is critical because it:
- enables manufacturers of chemical disinfectant products to choose the appropriate laboratory methods to support efficacy claims,
- enables end users of chemical disinfectant products to assess the information provided by the manufacturer and
- supports regulatory authorities in assessing claims made by manufacturers of disinfectant products.
No standardised method for testing a UV-C machine intended for the disinfection of semi-critical devices has been published. Manufacturers of UV-C machines are using the standard methods within the EN 14885 to demonstrate the effectiveness of their systems. However, these standards were developed specifically for chemical disinfection systems. They include practical methods that simulate how chemical products are intended to be used in a real-world application and include microorganisms that are explicitly challenging for chemical disinfectants.
UV-C machines are not chemical systems. Existing test methods within EN 14885 are not designed for non-chemical products, which inevitably leads to the UV-C manufacturers modifying these methods to suit their products. When deviations from the standard methods are made, the benefits of standardisation are lost, and we are left with no assurance that the product has been challenged appropriately.
The EN 148852 states:
‘In certain cases, it can be necessary or recommendable to modify even the test organism(s) to match the requirements of the area. Conformity to the standard used shall not be claimed, but it should be stated that the product was tested in accordance with the principles of the standard.'
‘Where there is no appropriate standard for an application within a specific area, a standard from another area may be recommended for use. If later on an appropriate standard is published, this new standard shall be used.’
The BS 8628 is the first of its kind and provides methods for quantitative testing of automated UV disinfection activities by direct illumination. This standard is now the most appropriate standard for testing UV machines intended for disinfection and is derived from the pre-existing standard EN 17272, which outlines methodologies for the microbiological efficacy testing of airborne disinfection processes/systems.
In this case, BS 8628 is the minimum we should expect from all UV-C machines claiming to high-level disinfect semi-critical medical devices on the market.
2. Compatibility
Plastic polymers make up a significant proportion of modern semi-critical devices. This includes ultrasound devices and endoscopes, which typically contain plastics such as Acrylonitrile Butadiene Styrene (ABS), Polypropylene (PP), Polycarbonate (PC), and Polyvinyl Chloride (PVC). These plastics offer a balance of properties such as mechanical strength, chemical resistance, flexibility, transparency, and ease of processing, making them suitable for various components and applications within ultrasound devices.
UV-C light has been shown to cause damage to plastics through consistent exposure. A recent study assessed the impact of UV-C light exposure on 10 plastic materials commonly used in healthcare. All materials showed degradation, however some plastics such as ABS and Polycarbonate showed evidence of significant surface damage.3 These materials are commonly used for device surroundings and casings.
It was concluded that: ‘exposure to UV-C should be limited for these types of materials as much as possible in healthcare facilities, especially where UV-C devices are routinely used’.
(Teska et al., 2020)3
3. Requirement for Manual Cleaning

Cleaning is regarded as the most critical step in the decontamination procedure.
‘Thorough cleaning is required before high-level disinfection and sterilization because inorganic and organic materials that remain on the surfaces of instruments interfere with the effectiveness of these processes.’
(Rutala and Weber, 2016)4
Ultimately, if the cleaning process is compromised, it is likely that the subsequent disinfection process will be adversely affected. Cleaning holds particular importance for UV-C systems, where no manual abrasion is used. If cleaning fails, soiling will persist even after exposure to UV-C disinfection, rendering the entire process ineffective. In contrast, manual processes like wiping, involves an additional abrasion step, facilitating the removal of any remaining soiling.
It is crucial to emphasise that cleaning agents must be thoroughly removed from the device prior to disinfection with UV-C, and the device should be completely dry before being placed in a UV chamber. Any residual surface moisture can hinder the delivery of the required UV dose to the surface.
4. Shadowing
UV light travels in a straight line, and objects obstructing its path can create shadows by preventing the passage of light. When UV light is blocked, it fails to reach specific areas during disinfection, posing a risk of inadequate disinfection in those regions.
Some ultrasound devices may have complex shapes or surface textures that create a challenge in achieving uniform exposure to UV light, potentially resulting in areas where disinfection will be unsuccessful.
Surface topography refers to the physical features of a surface/device and includes complexities such as indentations, contours, textures, and any irregularities in shape. These complexities can block the light from reaching the surface beneath, causing shadowing. Most chemical products will not have an issue reaching these areas as additional attention can be paid by the user. Products such as foams may even get into surface scratches where pathogens reside.
In contrast to alternative disinfection methods, UV-C disinfection offers limited penetration depth. Consequently, it cannot effectively penetrate solid or liquid residues that may persist on surfaces with equal intensity. Therefore, if any soiling or moisture remains on a surface prior to UV-C exposure, the light will not reach all areas for disinfection, potentially leaving spots where microorganisms could persist.
Example:
UV disinfection is commonly employed for disinfecting organic fruit produce. A study evaluated how the surface roughness of fruit impacts the effectiveness of UV-C treatment. Fruits like apples, which have smoother surfaces, were shown to have significantly higher reductions in organisms compared to those with more intricate surfaces, such as peaches, raspberries, and even pears. It was concluded that this was down to the subtle roughness of the fruit surface compared to that of an apple. The premise of this study applies to all surface types. Ultimately, surfaces with varying textures or complexities are anticipated to pose a challenge for light exposure, making it difficult for light to reach all areas of the surface. (M.S. Roopesh et al., 2012)5
Surface scratches on older, used devices can equally contribute to the effect of shadowing. UV-C radiation is capable of damaging plastics integral to ultrasound devices, and this raises concerns about potential surface cracking with prolonged exposure. Such cracks could exacerbate the risk of shadowing, potentially shielding harmful pathogens from disinfection.
5. Other Areas of the Probe and Global Guidance

UV systems typically do not address the entire device, including the probe cable, plug, holder, and machine. Published literature has shown that these areas can become readily contaminated with pathogenic microorganisms.
‘Probe cords and machine keyboards present significant sources of infection, and this can include potential pathogens.’
(Westerway et al., 2017)6
UV systems are designed solely to disinfect the portion of the probe that come into contact with the patient. This does not consider the possibility that staff performing the procedure may come into contact with other areas of the device during a patient procedure, inadvertently causing cross-contamination. These areas should be considered equal to the insertable portion of the device and be disinfected to the same level, which is not possible with most UV systems.
Guidance:
World Federation for Ultrasound in Medicine and Biology (WFUMB) – Guidelines for Cleaning Transvaginal Ultrasound Transducers Between Patients, 2017 states: ‘An additional consideration is the fact that the transducer handle and cable can also become contaminated and may also require disinfection.’ (Abramowicz et al., 2017)7Also, the Infection Prevention and Control in Ultrasound. Best Practice Recommendations from the European Society of Ultrasound Working Group, 2017 states:‘Thorough decontamination of US transducers and any equipment in direct patient contact before and after every patient, to the level required for specific procedures and in compliance with manufacturer specifications to avoid transducer surface damage, should be carried out.This includes regular decontamination of US keyboard/ console and any cables.’‘All US equipment in direct or indirect patient contact must be thoroughly cleaned and disinfected at the start of the examination and after every patient. This includes the US transducer with handle, cable and transducer holder (as far as possible) as well as additional devices which may be used during diagnostic or interventional procedures such as US fusions sensors/cables…Contamination of US equipment may be underestimated.’
(Nyhsen et al., 2017)8
6. Repair Mechanisms
Example:A study has shown that as much as 60% of microorganisms originally killed with UV-C can be reversed.(Song, Mohseni and Taghipour, 2019)9This study was conducted with E. coli but many other bacteria contain enzymes and repair mechanisms that may allow for photoreactivation and photorecovery from UV exposure.(Kowalski, 2009)10




-205x205.jpg)




